65 Yr old male with DKA with community acquired pneumonia and prerenal AKI
Hello all this is J. Mounika, a nineth semester student.This E Log depicts the patient centered approach to learning
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Consent: An informed consent has been taken from the patient in the presence of the family attenders and other witnesses as well and the document has been conserved securely for future references
A 65 year old male was brought to casualty with
CHIEF COMPLAINTS
Fever since 4 days
Breathlessness since 1 day
HISTORY OF PRESENTING ILLNESS
Patient was apparently asymptomatic 10 days back when he developed cold and cough with expectoration which is greenish and mucoid. Now the expectoration has decreased.
Then developed fever 4 days back which is high grade, continuous and not associated with chills and rigor.
Complaints of decreased appetite since 3days
And shortness of breath since 1 day - grade - II now increased to grade - IV since last night.
H/o nausea but no vomiting
No H/o decreased urine out put, pedal edema, loose stools
DAILY ROUTINE
He is a shopkeeper by occupation according to the attender his daily routine is as follows6 am: takes a cup of tea with sugar
6:30 am: he opens his shop
If he takes a breakfast it's b/w 7-7:30 am
9 am: takes a cup of tea with sugar
11 am: bathes and goes to his shop again
12:30 pm: he eats his lunch
6:00 pm: takes a cup of tea with sugar
7:30 pm: takes his dinner which consist of rice
9 pm: he sleeps
PAST HISTORY
N/K/C/O DM, HTN, TB, Epilepsy, CVA, CAD
Complaints of pain in bilateral knee joints for which he takes NSAIDS when pain increases.
H/o Surgery for right tibial fracture 5 years back
PERSONAL HISTORY
Diet : Vegetarian
Appetite : Normal before 3 days
Sleep: adequate
Bowel and bladder : regular
Addictions : used to smoke but stopped 5 years back
FAMILY HISTORY
Not significant
GENERAL EXAMINATION
Patient conscious and coherent co-operative


VITALS
Pulse : 98bpm
RR : 21 cpm
BP : 90/60 mm Hg
Temp. : 99°F
SpO2 : 96%
SYSTEMIC EXAMINATION
CVS : S1, S2 hear, no thrills and murmurs
Rs : position of trachea - central
BAE +, NVBS +
decreased breath sounds in infra axillary and mammary area
Dysnea, wheeze, rales and ronchi - absent
Abdomen: scaphoid shaped, soft and diffuse tenderness
CNS:
Slurred speech
No neck stiffness
Tone : Normal in both the limbs
Power : 4/5 in both the limbs
Reflexes : Right Left
Biceps ++ ++
Triceps ++ ++
Supinator + +
Knee ++ ++
Ankle ++ ++
Plantar Flexor Flexor
Cerebellar examination : normal
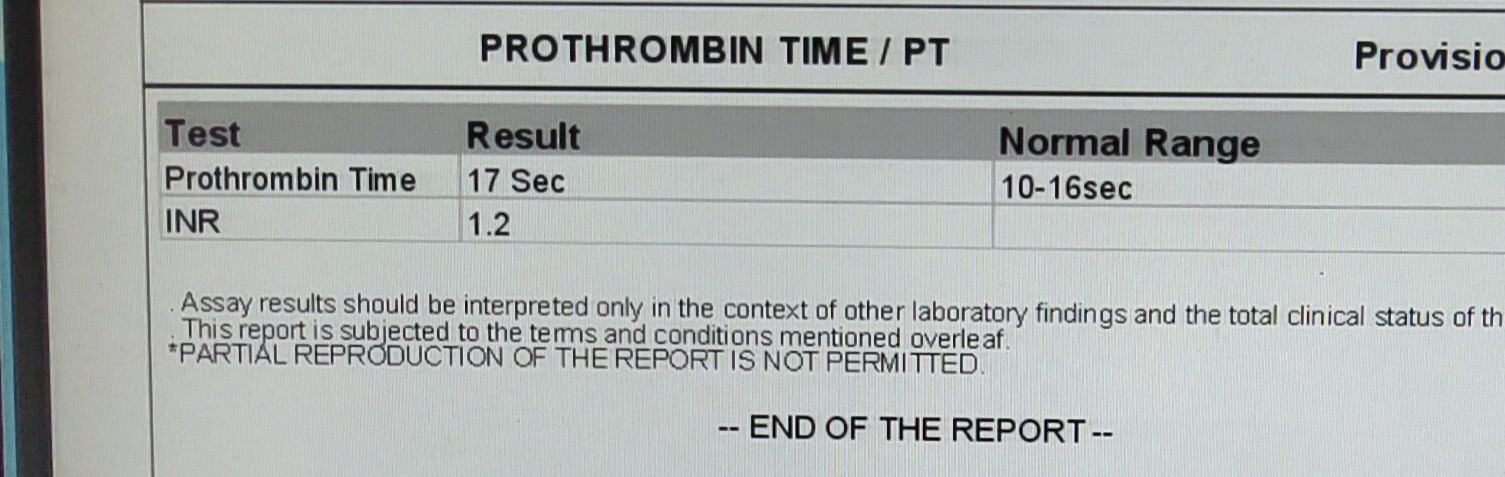
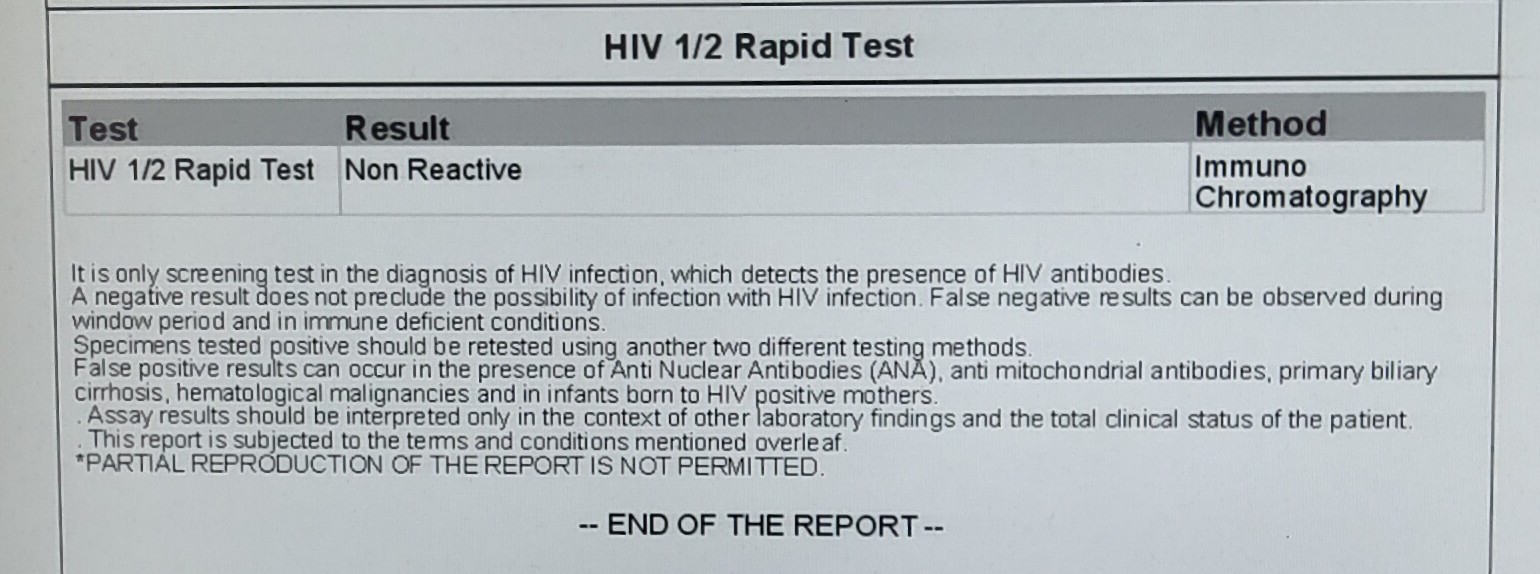
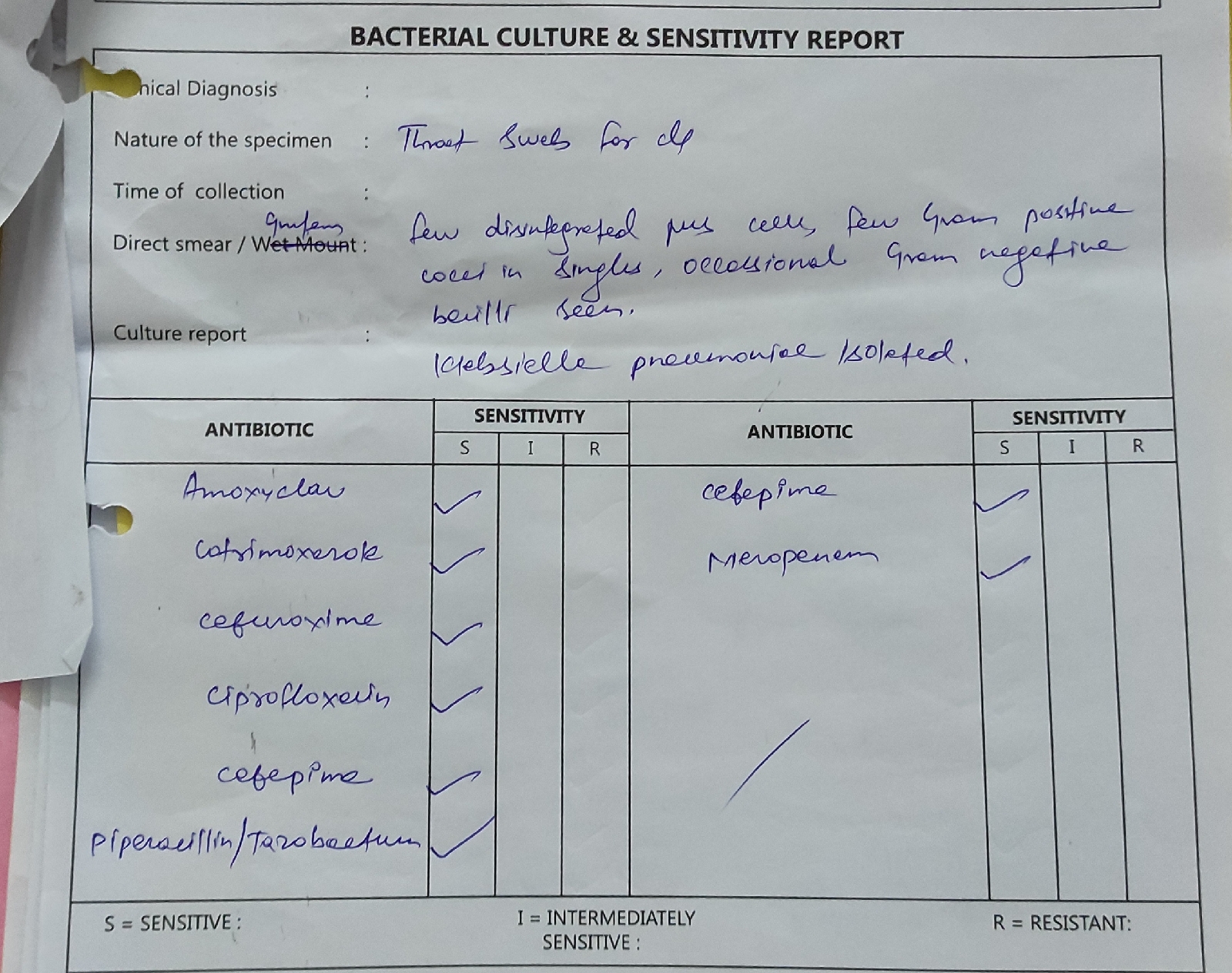
INVESTIGATIONS
























USG

GBS Charting

On 05/12/2023


Provisional Diagnosis:
Diabetic ketoacidosis with community acquired pneumonia with prerenal AKI.
TREATMENT
2/12/2023
1) NBM until further orders
2) IV Fluids NS @ 100ml/hr
3) Inj. PIPTAZ 2.5gm IV/TID
4) Inj. LINEZOLID 600mg IV/BD
5) Tab. AZITHROMYCIN 500mg OD
6) Tab. FLUCONAZOLE 150 mg OD
7) Inj. HOMAN ACTRAPID INSULIN infusion @ 6units/hr
8) Inj. PCM 18g IV/SOS ( if temp. >= 101°F)
9) Inj. LASIX 20mg IV/BD ( if SPB >= 110)
10) IV Fluids - FRUSIDEX @ 50ml/hr
11) Tab. ATORUAS 40mg OD
12) Tab. CLOPITAB - A75/75 OD
13) Inj. PAN 40mg IV/OD
14) GRBS moniter hourly
15) Moniter BP, PR, RR, SPO2 Hourly
8:40 PM
1) Stop insulin infusion
2) Inj. HAI 6U in 500ml DNS over 5hrs
3) Inj. KCL 20mEq in 500 NS over 5hrs
Followed by
4) Inj. KCL 20mEq in 500 NS over 5hrs
5) GRBS moniter hourly
3/12/2023
1) Inj. PIPTAZ 2.25gm IV/TID
2) Inj. LINEZOLID 600mg IV/BD
3) Tab. AZITHROMYCIN 500mg OD
4) Tab. FLUCONAZOLE 150 mg OD
5) Inj. PAN 40mg IV/OD
6) Inj. PCM 1g IV/SOS ( if temp. >= 101°F)
7) Inj. LASIX 20mg IV/BD ( if SPB >= 110)
8) Inj. HOMAN ACTRAPID INSULIN infusion S/L TID according to GRBS
9) Tab. ATORUAS 40mg OD
10) Tab. CLOPITAB - A75/75 OD
11) GRBS moniter 2 hourly
12) Moniter BP, PR, RR, SPO2 2 Hourly
13) Nebulization with IPRAVENT 8th hourly and BUDECORT 12th hourly
14) Inj. KCL 20mEq in 500 NS over 5hrs
15) Tab. FENOFIBRATE 160mg OD
16) Tab. METOPROLOL 25mg OD
17) IV fluid DNS with 6u HAI + 20mEq KCl at 100ml/hr
4/12/23
1) Inj. PIPTAZ 2.25gm IV/TID
2) Inj. LINEZOLID 600mg IV/BD
3) Tab. AZITHROMYCIN 500mg OD
4) Tab. FLUCONAZOLE 150 mg OD
5) Inj. PAN 40mg IV/OD
6) Tab atorvas 20 MG OD
7)tab metaprollel 25 mg oral OD
8) tab fenofibrate 160 MG OD
9) tab sporolac oral OD
10)Inj.calcium gluconate IV
11)Neb. Budecort inhaler
05/12/23
1) Inj. PIPTAZ 2.25gm IV/TID
2) Inj. LINEZOLID 600mg IV/BD
3) Tab. AZITHROMYCIN 500mg OD
4) Tab. FLUCONAZOLE 150 mg OD
5) Inj. PAN 40mg IV/OD
6) Tab atorvas 20 MG OD
7)tab metaprollel 25 mg OD
8) tab fenofibrate 160 MG oral OD
9) tab sporolac oral OD
10)Alkastone syrup

Comments
Post a Comment