gm e-log
A 52 year old female patient came with chief complaints of pedal edema since 1 month and nausea and vomiting since 10 days.










HISTORY OF PAST ILLNESS
patient was apparently asymptomatic six months back and then on routine checkup she was found to have kidney problem .
-from one month she developed pedal edema and gradually progressing which is of bilateral pitting type extending upto knees.
-vomiting from 10 days associated with nausea and decreased appetite
HISTORY OF PAST ILLNESS
no history of SOB
k/c/o type 2 Diabetes mellitus since 10 years.
TREATMENT HISTORY
have taken treatment for diabetes from 10 years
PERSONAL HISTORY
• She is unmarried.
• She has decreased appetite.
• Has regular bowels
• Has normal micturition.
• No known allergies and addictions
FAMILY HISTORY
-not significant.
ON EXAMINATION :
-Patient is conscious, coherent, cooperative.
- pallor , Icterus,clubbing, cyanosis lymphadenopathy are absent.
-malnutrition, edema present.
Vitals :
• BP - 140/80 mmHg
• Temp. - 98.6°
• SpO2 - 97%
• RR - 18 cycles/min
• PR - 82 bpm
Systemic Examination:
CVS:
• S1, S2 heard
• No thrills and cardiac murmurs
RESPIRATORY SYSTEM:
• No dyspnoea, wheezing
• Postion of trachea - central
• Breath sounds - Vesicular
ABDOMEN:
• No tenderness, palpable mass, bruits
• No palpable liver and spleen
CNS:
• Conscious and coherent
• Speech - normal
• No signs of meningeal irritation
• Glass gow coma scale - 15/15
PROVISIONAL DIAGNOSIS:
CKD?
Diabetic nephropathy with severe anaemia
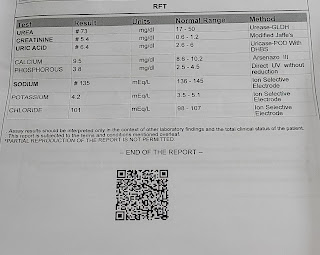
INVESTIGATIONS
Treatment:
Fluid restriction <1.5L /day
Salt restriction <2gm/day
TAB. LASIX 40mg BD
TAB. NODOSIS 500 mg BD
TAB OROFER -XT OD
INJ. ERYTHROPOIETIN
GRBS 7-1-7-20
INJ. H. ACTRAPID acc.to GRBS
HEMODIALYSIS


Comments
Post a Comment